Finasteride, dutasteride, RU58841, and saw palmetto all target the same pathway: they lower dihydrotestosterone (DHT) levels or block its receptor. Minoxidil can extend the anagen (growth) phase of hair follicles.Yet many users continue to lose density and experience recession, indicating that DHT is only one factor in pattern hair loss.
PGD₂: The Surprise Co-Conspirator
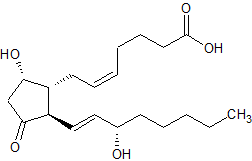
Back in 2012, a Penn dermatology team compared “hairy” and “bald” punch biopsies from the same scalps. In the bald zones they found triple the level of prostaglandin D₂ (PGD₂) and a surge in its maker enzyme, PTGDS. When they drenched cultured follicles—or even shaved mice—in PGD₂, growth simply stopped. The more PGD₂, the shorter the hair.
Chemically, PGD₂ slots into the CRTH2/DP2 receptor on follicle cells, flicking on an inflammatory circuit that hustles hairs out of their growth phase. Think of DHT as the arsonist and PGD₂ as the accelerant—it doesn’t start the fire, but it makes sure the building burns.
Big Pharma’s Airball on Inhibiting PGD₂
Asthma companies already had DP2 antagonists on the shelf, so repurposing looked easy money.Oral DP2 antagonists—setipiprant, fevipiprant, and timapiprant—were repurposed from asthma pipelines but never delivered clinical gains. Setipiprant failed a 24-week, 169-subject trial, showing hair counts no better than placebo. Fevipiprant and timapiprant never even started scalp studies after lukewarm asthma data and looming patent expirations. The common lesson: oral dosing keeps blood levels safe for the lungs but too low to saturate follicles, and pushing the dose high enough would raise systemic-safety flags.
| Drug (route) | What happened in AGA? | Post-mortem |
|---|---|---|
| Setipiprant (oral) | 169 men, 24 weeks—no better than placebo | Blood levels safe for lungs never reached follicles oaicite:1 |
| Fevipiprant, Timapiprant (oral) | Never reached a scalp trial | Ho-hum asthma data, patents expiring oaicite:2 |
Moral: a systemic pill can’t fix a problem parked inside an oil-gland funnel unless the dose goes hair-raisingly high, which regulators (and livers) dislike.
Over-The-Counter Underdog: Topical Cetirizine Front and Center
Cetirizine—the familiar non-drowsy allergy pill—can be compounded into a 1 % scalp solution that down-regulates PTGDS, lowers PGD₂, and nudges “pro-growth” PGE₂ upward. In a 16-week single-blind pilot of 40 men, topical cetirizine raised total and anagen hair counts to about the same level achieved by 5 % minoxidil (PubMed). A 24-week double-blind study in 66 women then paired cetirizine with minoxidil and reported thicker shafts, denser vertex coverage, and higher self-ratings than minoxidil plus placebo (PubMed).
Why Topical Cetirizine Succeeds Where Oral DP2 Blockers Falter
Why might cetirizine show traction when oral DP2 antagonists stalled? Three plausible reasons:
Local delivery, higher follicular exposure. A 1 % solution can sit in sebum and diffuse directly into the follicle sheath, achieving concentrations oral drugs never reach without systemic-safety trade-offs.
Dual prostaglandin shift. Cetirizine not only dampens PGD₂ by suppressing PTGDS but also modestly increases PGE₂, a prostaglandin linked to anagen maintenance. The oral DP2 blockers only blocked the receptor, leaving the overall PG balance unchanged.
Extra anti-inflammatory benefit. As an H₁ antihistamine, cetirizine calms mast-cell activity and scalp itch—secondary effects that may further reduce micro-inflammation around miniaturising follicles.
Put together, cetirizine delivers more drug exactly where it matters, nudges the prostaglandin balance in two directions, and adds a layer of anti-inflammatory support—advantages the first-generation oral antagonists simply didn’t have.
Cetirizine’s Off-Label Role in Custom Hair Treatments
Because cetirizine is already FDA-approved for allergies, pharmacies may legally compound it, and tele-derm services—Roots by GA among them—let physicians slot the molecule into personalised cocktails alongside minoxidil, finasteride, or latanoprost Roots. That doesn’t make cetirizine `a certified hair-loss cure—large, head-to-head studies are still missing—but the early data highlight a simple principle: when you shut PGD₂ down right at the follicle, the follicle listens.
Synergistic Treatment: Hormones, Growth, Inflammation
A credible protocol might stack:
Hormone control – dutasteride, finasteride, alongside anti-androgen treatments.
Growth push – minoxidil, microneedling, exosome cocktails.
Inflammation brake – cetirizine now; bespoke DP2 or PTGDS inhibitors later.
Addressing all three fronts is likely to produce better, longer-lasting results than focusing on DHT alone.
DHT is still central to androgenetic alopecia, but it does not act in isolation. Elevated PGD₂ levels add an inflammatory signal that keeps follicles cycling out of growth even when DHT is suppressed. Early setbacks with oral DP2 antagonists showed that systemic delivery isn’t enough; treatment has to reach the follicle. Topical cetirizine gives the first proof of concept, and next-generation DP2 or PTGDS inhibitors may refine the approach further.